
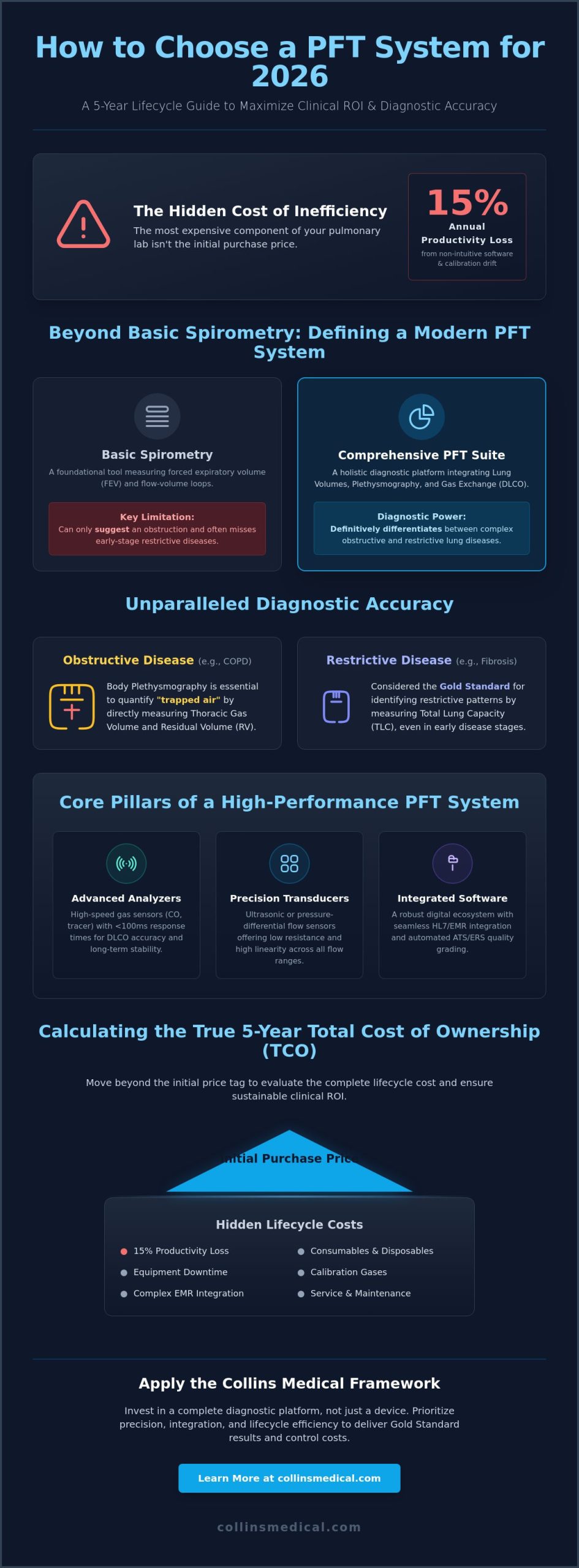
The most expensive component of your pulmonary lab isn’t the initial purchase price; it’s the 15% annual productivity loss caused by non-intuitive software and recurring calibration drift. Knowing how to choose a pft system for 2026 requires looking beyond the spec sheet to evaluate how a device performs over a five-year clinical lifecycle. Whether you’re managing a facility in MA 01747 or Ashford, Kent, the pressure to deliver Gold Standard results while controlling costs has never been higher.
You likely agree that equipment downtime and complex EMR integration are more than just technical hurdles; they’re barriers to patient care that drain your budget. This article provides a comprehensive framework for healthcare administrators and clinicians to evaluate pulmonary function testing technology based on precision, software integration, and lifecycle efficiency. We’ll explore how to achieve unparalleled diagnostic accuracy, minimize total cost of ownership, and ensure your data flows seamlessly into hospital HL7 systems.
Key Takeaways
- Distinguish between basic spirometry and comprehensive PFT suites to ensure your facility can accurately differentiate between obstructive and restrictive lung diseases.
- Master how to choose a pft system by prioritizing analyzer linearity and self-linearizing technology to maintain clinical precision across diverse patient populations.
- Reduce operational downtime through advanced digital ecosystems that offer seamless software integration and revolutionary remote diagnostic capabilities.
- Move beyond initial purchase prices to accurately calculate the five-year Total Cost of Ownership (TCO), including essential consumables and calibration gases.
- Apply the Collins Medical Framework to select the ideal mobile or fixed-mount configuration, supported by our expert service hubs in MA 01747 and Kent TN23 1LY.
Defining the Modern PFT System: Beyond Basic Spirometry
A common mistake in clinical procurement is conflating a standalone spirometer with a complete pulmonary lab. While spirometry remains a foundational tool for measuring forced expiratory volume, 2026 diagnostic standards demand a more holistic approach. Understanding the technical breadth of Pulmonary Function Testing (PFT) is essential when evaluating how to choose a pft system for high-volume clinics or research facilities. A modern system must integrate lung volumes and gas exchange capabilities to provide a definitive clinical picture.
Clinicians today require equipment that offers more than just flow-volume loops. High-performance systems integrate advanced hardware with sophisticated software to automate biological calibration and ensure data integrity. These systems allow providers to move beyond simple screening and into the territory of complex differential diagnosis. This shift is driven by the need for precision in identifying early-stage pathologies that basic volume measurements often miss. For those interested in the technical progression of these devices, exploring our legacy of pulmonary excellence provides context on how these systems have evolved from bulky analog units to the streamlined digital suites used today in MA 01747 and Kent TN23 1LY.
Obstructive vs. Restrictive Diagnostic Requirements
Advanced PFT systems are critical for distinguishing between obstructive conditions like COPD and restrictive diseases such as pulmonary fibrosis. While spirometry can suggest an obstruction, it can’t accurately quantify the “trapped air” seen in emphysema. Comprehensive systems utilize body plethysmography to measure thoracic gas volume directly. Plethysmography is the gold standard for lung volume measurement in clinical settings. By determining Total Lung Capacity (TLC) and Residual Volume (RV), clinicians can identify restrictive patterns that are often masked by normal spirometry results in early disease stages.
The Evolution of Gas Exchange Testing (DLCO)
Diffusing capacity of the lungs for carbon monoxide (DLCO) is the most sensitive indicator of early interstitial lung disease. Modern 2026 standards require gas analyzers with response times under 100 milliseconds to ensure accuracy during the brief breath-hold maneuver. Fast-responding analyzers don’t just improve data precision; they significantly enhance patient comfort by reducing the effort required for repeatable tests. When clinicians analyze how to choose a pft system, the speed and stability of the infrared or electrochemical gas sensors should be a primary technical priority.
Core Components of High-Performance Systems
A robust PFT suite consists of three primary pillars that must work in perfect synchronization:
- Analyzers: High-speed gas sensors for CO and tracer gases that maintain stability over long clinical shifts.
- Transducers: Ultrasonic or pressure-differential flow sensors that offer low resistance and high linearity across all flow ranges.
- Integrated Software: Platforms that support HL7 and EMR integration, providing real-time quality grading based on the latest ATS/ERS 2019/2024 standards.
By focusing on these core components, facilities ensure they aren’t just buying a device, but investing in a diagnostic platform capable of meeting the rigorous demands of modern respiratory medicine.
Technical Evaluation: Accuracy, Linearity, and Analyzer Technology
Precision isn’t just a metric; it’s the foundation of every respiratory diagnosis. When clinical directors evaluate how to choose a pft system, the analyzer’s ability to maintain linearity across diverse patient profiles remains the top priority. High-volume clinics processing 25 or more patients daily can’t afford the data drift associated with aging sensors. Reliability ensures that a patient’s results remain comparable over a five-year treatment plan, providing a clear picture of disease progression or recovery.
Fast, reliable results drive the efficiency of modern pulmonary departments. If an analyzer requires frequent re-testing due to inconsistent readings, the clinical workflow collapses. Sensors must provide long-term data consistency to meet the rigorous demands of multi-site clinical trials and daily diagnostic rounds. Choosing a system with durable hardware reduces the frequency of sensor replacements, directly lowering the total cost of ownership over a typical 7-year equipment lifecycle.
The Science of Self-Linearizing Gas Analyzers
Manual calibration consumes valuable staff time and introduces the risk of human error. Modern self-linearizing technology automates this process, ensuring the system meets the 2019 ATS/ERS technical standards without constant technician intervention. This stability reduces gas consumption by approximately 20% to 30% because the system doesn’t require frequent, wasteful purging cycles. Adhering to established Clinical Guidelines for PFT ensures your lab stays compliant while maximizing patient throughput. Collins Medical engineers these automated solutions to support busy labs from our headquarters in MA 01747 and our UK base in Ashford, Kent, TN23 1LY.
Sensor Technology and Data Integrity
The choice between ultrasonic and pressure-differential sensors significantly impacts long-term maintenance. Ultrasonic sensors offer a “no-moving-parts” advantage, which is crucial for maintaining accuracy in pediatric and geriatric patients who may exhibit very low flow rates. The precision of the flow sensor determines the exact moment of peak flow, which directly dictates the accuracy of the FEV1 calculation by measuring the volume exhaled during the first second of a forced maneuver. High-volume environments require sensors that resist moisture and debris to prevent data degradation during back-to-back testing sessions. When you’re deciding how to choose a pft system, prioritize sensors that demonstrate stability across the entire flow range, from 0.05 L/s to 16 L/s.
The Digital Ecosystem: Software Integration and Remote Servicing
Deciding how to choose a pft system for a 2026 clinical environment starts with the digital interface. Software is no longer just a data collector; it’s the primary engine of diagnostic efficiency. Modern proprietary platforms must balance ease of use with robust data management. Collins Medical leverages its legacy of pulmonary excellence to develop software that simplifies complex ATS/ERS 2019 reporting. These systems turn raw flow-volume loops into clear, actionable reports. This allows clinicians to focus on patient care rather than navigating complex sub-menus.
Administrative burdens often slow down busy pulmonary labs. Automated data entry and cloud-based review platforms address this directly. By moving to a digital-first workflow, facilities can reduce the time spent on manual documentation by approximately 20 minutes per physician every day. This shift doesn’t just improve morale; it increases patient throughput by 12% on average across high-volume clinics.
HL7 and EMR Interoperability
Seamless integration with hospital EMRs is a non-negotiable requirement for 2026. Manual data entry errors account for roughly 15% of clinical documentation mistakes in respiratory departments. HL7 upgrades allow for real-time data synchronization across hospital networks, whether you’re operating in Ashford, Kent (TN23 1LY) or MA 01747. This connectivity ensures that respiratory data is instantly available in the patient’s electronic record. Security remains paramount. Systems must utilize TLS 1.3 encryption and adhere to SOC 2 Type II standards to protect sensitive patient data in a connected environment.
Remote Servicing and Real-Time Troubleshooting
The “downtime objection” used to be the primary fear for lab managers. Remote diagnostic capabilities have revolutionized PFT maintenance. Technicians can now resolve 85% of software glitches and calibration issues through secure remote access. This eliminates the need for most on-site visits and reduces clinical downtime by an average of 48 hours per incident. It’s a critical factor when determining how to choose a pft system that maximizes operational uptime. Modern service contracts include proactive system monitoring and automated firmware updates. These tools ensure your equipment performs at peak accuracy 365 days a year without requiring constant manual intervention from your IT staff.
- Reduces manual entry errors by up to 15% through HL7 automation.
- Minimizes downtime with 85% of issues resolved via remote diagnostics.
- Enhances physician efficiency with cloud-based remote data review.
- Protects patient privacy with modern TLS 1.3 encryption protocols.
Calculating Total Lifecycle Costs and Clinical ROI
Buying medical equipment isn’t just about the initial invoice. For labs figuring out how to choose a pft system, the Total Cost of Ownership (TCO) represents the real financial commitment. A 2023 industry study found that initial purchase costs often account for only 40% of the total expenditure over a seven-year period. The remaining 60% is tied to consumables, maintenance, and operational downtime. Clinicians can review our legacy of pulmonary excellence to understand why precision impacts these long-term costs.
Consumables and Maintenance Budgeting
High-quality PFT filters and sensors are non-negotiable for hygiene and clinical accuracy. While third-party alternatives might seem cheaper, using non-OEM parts can void manufacturer warranties and lead to drift in sensor calibration. Labs should budget for gas analyzer replacement cycles every 24 to 36 months depending on patient volume. Standard 5-year projections must include the rising cost of medical-grade calibration gases and the disposal of single-use components. Understanding these long-term variables is vital when deciding how to choose a pft system that remains profitable for its entire lifespan.
- Filters: Essential for preventing cross-contamination and protecting the internal flow sensor from moisture.
- Calibration Gases: Requires consistent budgeting for specialty mixtures like CO and Helium.
- Sensors: Electrochemical or ultrasonic sensors have different replacement schedules that impact the annual budget.
Operational Efficiency and Patient Throughput
System speed directly dictates revenue. Modern systems with automated daily calibration and rapid gas washout periods can shave 8 to 12 minutes off each testing session. This efficiency reduces the “dead time” between patients. Better patient feedback interfaces on the technician’s screen also lower the rate of test re-runs. A 10% increase in patient throughput, achieved through faster gas stabilization and intuitive software, can generate an additional $45,000 in annual revenue for a typical pulmonary clinic.
Advanced diagnostic software reduces coding errors by providing clear, standardized reports that align with current procedural terminology (CPT) requirements. This precision minimizes claim denials and speeds up the reimbursement cycle. When systems integrate directly with EMR platforms, the administrative time spent on manual data entry is virtually eliminated, allowing staff to focus on patient care rather than paperwork.
Ready to optimize your lab’s performance? Request a personalized quote for a high-ROI PFT system from our experts in Massachusetts or Kent.
Implementation and Selection: The Collins Medical Framework
Choosing a PFT system requires balancing clinical precision with operational reality. Facility managers must decide between fixed-mount stations for high-volume laboratories and mobile solutions for versatile bedside testing. This choice dictates workflow efficiency and patient throughput for years. Understanding how to choose a pft system involves evaluating the hardware and the long-term reliability of the manufacturer. When you decide how to choose a pft system, the support infrastructure is as vital as the sensor technology itself.
Global Support with Local Expertise
Collins Medical operates through two primary centers of excellence to ensure rapid technical response. North American operations are centered at the headquarters in Hopedale, Massachusetts (MA 01747). This site handles sales, parts distribution, and expert consultation for the US market. European and UK clients receive dedicated support from the Ashford, Kent (TN23 1LY) facility. Partnering with a legacy brand means accessing nearly 100 years of innovation in pulmonary health. You aren’t just buying a machine; you’re securing a decade of uptime through local expertise.
The Eagle 3 Advantage
The Eagle 3 represents a shift in how respiratory diagnostics are managed. It integrates self-linearizing analyzers that maintain accuracy without constant manual intervention. Remote servicing capabilities allow technical teams to diagnose software issues without a site visit, which can reduce downtime significantly in busy clinical settings. These features ensure the system remains compliant with the latest ATS/ERS standards without placing an undue burden on your biomedical staff.
Mounting options are flexible. You can choose compact configurations for space-constrained clinics or full-scale lab setups for major hospitals. The system adapts to your floor plan rather than forcing you to renovate. To move forward, request a site-specific workflow assessment or a personalized quotation. This ensures the equipment matches your specific patient volume and diagnostic goals. You can experience the future of PFT with Collins Medical by reviewing our legacy of innovation and technical specifications.
- Fixed-Mount: Ideal for dedicated pulmonary labs requiring maximum stability and integrated seating.
- Mobile Solutions: Best for multi-department use or facilities with limited square footage.
- Direct Support: Access engineers directly in MA 01747 or Kent TN23 1LY to minimize service delays.
Future-Proofing Your Lab with Next-Generation PFT Technology
Deciding how to choose a pft system for 2026 requires balancing technical precision with long-term operational viability. Clinical leaders must prioritize hardware that eliminates measurement drift. The Eagle 3 utilizes self-linearizing gas analyzers to maintain unparalleled accuracy without the need for constant manual recalibration. This level of precision is vital for longitudinal patient tracking and reliable diagnostic outcomes. Beyond the hardware, the digital shift necessitates systems that support remote servicing. This capability reduces clinical downtime by identifying and resolving software issues before they disrupt daily patient flow.
Collins Medical brings a legacy of pulmonary excellence dating back to the 1930s. This history provides a foundation of reliability for modern respiratory departments. By focusing on the Collins Medical Framework, labs secure a system that integrates into HL7 ecosystems while minimizing total lifecycle costs. Whether you’re operating out of Ashford, Kent, TN23 1LY, or managing a facility near MA 01747, selecting a partner with deep industry roots ensures your investment remains at the cutting edge. It’s time to elevate your diagnostic capabilities with technology built for the next decade of respiratory care.
Request a Personalized Quote for the Eagle 3 PFT System
Your team deserves the confidence that comes with world-leading respiratory technology and a partner dedicated to your clinical success.
Frequently Asked Questions
How often should a professional PFT system be calibrated for clinical accuracy?
Clinical standards from the ATS and ERS mandate that you perform a volume calibration check every day of testing using a certified 3L syringe. Gas analyzers and pressure transducers typically require calibration before each patient session or at least every 4 hours of continuous use. Maintaining these 2019 updated standards ensures your results remain within the required 2.5% accuracy range for diagnostic reliability.
What is the difference between a portable spirometer and a full PFT system?
A portable spirometer measures basic flow and volume, whereas a full PFT system provides a comprehensive diagnostic suite including DLCO and lung volumes. Full systems utilize specialized gas analyzers and often include a plethysmography cabin to measure functional residual capacity. While handheld units are excellent for bedside screenings, full systems deliver the 360 degree data needed for complex differential diagnoses in a clinical laboratory.
Can modern PFT systems integrate with our existing Epic or Cerner EMR?
Modern PFT systems use HL7 and DICOM protocols to facilitate seamless bi-directional integration with major EMR platforms like Epic and Cerner. This connectivity allows patient demographics to flow directly to the equipment and pushes completed test results back to the patient record instantly. Implementing these digital workflows reduces manual data entry errors by 40% and speeds up the physician review process.
What are the essential CPT codes associated with pulmonary function testing in 2026?
The primary CPT codes for respiratory diagnostics include 94010 for basic spirometry, 94726 for plethysmography, and 94729 for DLCO gas exchange analysis. If you’re performing pre and post bronchodilator studies, you’ll use code 94060. Accurate application of these codes is critical for ensuring your facility receives full reimbursement for the technical and professional components of the testing.
Is remote servicing secure for medical devices under HIPAA or UK GDPR?
Remote servicing is highly secure when conducted through encrypted 256-bit VPN tunnels that meet both HIPAA and UK GDPR requirements. Technical teams based in MA 01747 and Kent TN23 1LY use these point-to-point connections to diagnose 85% of software issues without needing an onsite visit. This approach maintains strict patient privacy while significantly reducing equipment downtime for the clinic.
How do self-linearizing analyzers reduce the cost of calibration gases?
Self-linearizing analyzers use advanced ultrasonic or rapid-response sensors to reduce calibration gas waste by 30% compared to older fuel cell technologies. These systems automate the linearization process, which means they don’t require the frequent multi-point gas adjustments that consume expensive cylinders. Over a five-year lifespan, this innovation can save a high-volume lab thousands in recurring consumable expenses.
What are the space requirements for a full plethysmography (body box) system?
A standard plethysmography system requires a dedicated floor footprint of approximately 1.5 meters by 1.5 meters. You should also plan for a 2.5 meter ceiling height and at least 1 meter of additional clearance to allow the cabin door to swing open fully. When you’re researching how to choose a pft system, it’s vital to measure your doorway widths to ensure the cabin can be moved into the room during installation.
Should we prioritize DLCO or lung volume measurement for a new clinic?
Most new clinics prioritize DLCO because it’s the primary tool for assessing gas exchange and identifying interstitial lung diseases. While lung volume measurement via plethysmography is the gold standard for diagnosing restrictive patterns, DLCO often provides the most immediate clinical utility for a broad patient base. Ideally, a modular system allows you to start with DLCO and add lung volume capabilities as your patient volume grows.
Disclaimer
Collins Medical LLC and Collins Medical Ltd are associated but separate Companies and are not associated to or born from the Collins Medical Inc or Collins Medical Practice or Collins Medical Dictionary or Collins Medical Equipment Group.

